Galapagos’ clinical program for filgotinib for RA
Galapagos is developing a highly selective JAK1 inhibitor, called filgotinib (formerly known as GLPG0634), for treatment of RA, which we believe will address a number of the limitations of existing RA therapies. In a human whole blood assay Galapagos demonstrated that filgotinib, with a 30-fold selectivity for JAK1 over JAK2, was more selective for JAK1 than any other compound known to us to be either approved for sale or in clinical development. Galapagos believes the high selectivity of filgotinib for JAK1 may allow for a positive efficacy profile, with an improved safety profile for filgotinib due to the improved selectivity over JAK2 and JAK3.
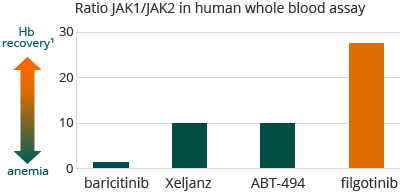

1 A. Tefferi, Blood 119 (2012) 2771-2730
Moreover, we believe that filgotinib has the potential to be used as a once-daily therapy, thereby potentially improving ease of administration and patient compliance. We also believe filgotinib has the potential to be used safely with concomitant medications, an important feature for this patient population since many of these patients are on other therapies to address co-morbidities or other diseases.
Through our DARWIN clinical programs, we demonstrated the following clinical and product effects of filgotinib for the treatment of RA:
- Safety profile: That filgotinib was well tolerated, showed absence of treatment-induced anemia, showed stable or improvement in the atherogenic index (percentage LDL versus HDL cholesterol) and resulted in an overall low infection rate and a favorable profile for liver enzymes
- Efficacy profile: That filgotinib enabled rapid onset of action, as measured by ACR20 response rates, with durable efficacy equal to or better than approved biologics and approaches such as anti-TNFs
- Convenience: That filgotinib enabled oral, once-daily dosing
- Combination with other therapies: That filgotinib will be able to be combined with other therapies commonly prescribed to RA patients, due to its low likelihood of drug-drug interactions
Filgotinib was evaluated in DARWIN 1 and 2 dose finding trials, Phase 2b trials in patients with moderate to severe RA and who have demonstrated an inadequate response to MTX. Patients completing one of these Phase 2b studies had the opportunity to roll-over to DARWIN 3, a long-term follow-up trial that allows patients to remain on treatment. The primary objective of the DARWIN 1 and 2 trials was efficacy in terms of percentage of subjects achieving an ACR20 response after 12 weeks of treatment. Final results after 24 weeks of treatment in both of the DARWIN trials were announced in July and August 2015, providing further insight as to the safety profile due to the fact the patients are treated for a longer period. Secondary trial objectives include efficacy in terms of the percentage of subjects achieving an ACR20 response at 24 weeks of treatment, ACR50 and ACR70 response and other disease activity measures as well as safety and tolerability and effects on subjects’ disability, fatigue and quality of life.
Below is an overview of the trial designs for the DARWIN clinical program.
Trial Name |
DARWIN 1 (GLPG0634-CL-203) |
DARWIN 2 (GLPG0634-CL-204) |
|---|---|---|
Trial Design |
Double-blind, placebo-controlled |
|
|
Add-on to MTX Seven trial arms:
|
Monotherapy Four trial arms:
|
|
Patient Population |
Subjects with moderately to severely active RA who have an inadequate response to MTX (oral or parenteral) |
|
Trial Objective |
Phase 2b dose finding trial to: |
|
|
|
|
|
||
Number of Subjects Randomized |
599 (594 treated) |
287 (283 treated) |
Total Treatment Duration |
24 weeks |
|
Re-Randomization |
At week 12, subjects on placebo or lower doses of filgotinib who have not achieved 20% improvement in swollen joint count, or SJC, 66, and tender joint count, or TJC, 68, are re-randomized automatically to another treatment arm with either a 50 mg or 100mg dose. Subjects in the other groups maintain their randomized treatment until week 24 |
|
Primary Trial Objective (at Week 12) |
Efficacy in terms of percentage of subjects achieving an ACR20 response of: |
|
|
|
|
Secondary Trial Objectives (at every visit) |
Efficacy in terms of the percentage of subjects achieving an ACR20, ACR50, ACR70, DAS28(CRP) and other disease activity measures Safety and tolerability Effects on subjects' disability, fatigue and quality of life of: |
|
|
|
|
|
Population PK and PD of filgotinib and its metabolite in subjects with RA and investigate the relationship between exposure and efficacy/safety/PD |
||
DARWIN 3 (GLPG0634-CL-205) is a multicenter, open-label, long-term follow-up safety and efficacy trial of subjects who have completed either DARWIN 1 or DARWIN 2. All subjects have started the trial at the same dose level, either at 200 mg once per day or at 100 mg twice per day (except for males in the U.S. sites of these trials who receive a maximum daily dose of 100 mg), depending on the regimen administered during the preceding trial, with DARWIN 1 subjects continuing to use filgotinib in combination with MTX.
In connection with the DARWIN clinical program, we agreed with the FDA to exclude the 200 mg filgotinib daily dose for male subjects; males receive a maximum daily dose of 100 mg in the U.S. sites in this trial. This limitation was not imposed by any other regulatory agency in any other jurisdiction in which the DARWIN clinical program is being conducted. See “Risk Factors–Risks related to product development, regulatory approval and commercialization.”
Measurements of RA
The severity of RA can be assessed using several indices as recommended by the ACR. The ACR criteria measure improvement in tender or swollen joint counts and include other parameters which take into account the patient’s and physician’s assessment of disability. These clinical disease activity parameters are combined to form composite percentages of clinical response that are known as ACR20, ACR50, and ACR70. An ACR20 score represents a 20% improvement in these criteria and is considered a modest improvement in a patient’s disease. An ACR50 score and ACR70 score represent a 50% and 70% improvement in the clinical response criteria, respectively, and each is considered evidence of a meaningful improvement in a patient’s disease.
Galapagos reported final 24 weeks’ data from DARWIN 1 in July 2015. DARWIN 1 was a 24-week, double-blind, placebo-controlled evaluation of filgotinib, as once- and twice-daily administration (QD and BID dosing, respectively) at three daily dose levels. Final results pertained to 594 patients with moderate to severe RA who showed an inadequate response to MTX and who remained on their background therapy of methotrexate. These patients received filgotinib or placebo and were evaluated up 24 weeks. Galapagos achieved the primary endpoint of ACR20 response at 12 weeks, reporting 80% ACR20 response on 100 mg BID versus 45% on placebo. We went on to report the following results for ACR50 response at 12 and 24 weeks:
ACR50 Responses
DARWIN 1, ITT-NRI
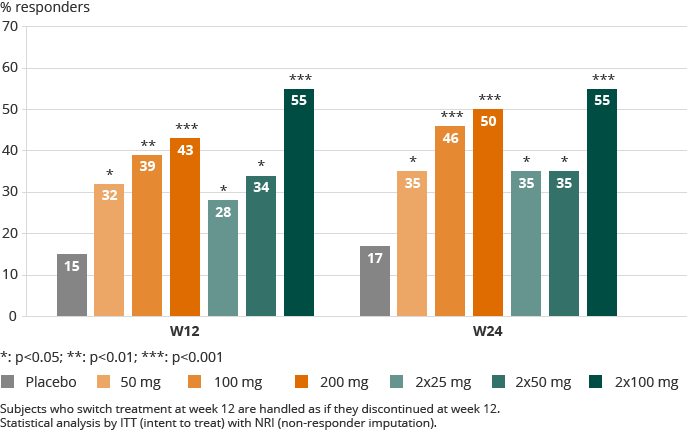

Overall, there was no statistically relevant difference between the once-daily and twice-daily dosing regimens.
Over all DARWIN 1 dose groups including placebo, 3.9% of patients stopped treatment during the study for safety reasons. Patients reporting serious (2.5% overall) and non-serious treatment-emergent adverse events were evenly spread over the dose groups including placebo. Serious infections were reported in six patients, including one death on active treatment in the second half of the study and for which the Data Safety Monitoring Board did not see a reason to pause or change the study. No opportunistic infections were reported. Herpes zoster infection occurred in five patients, equally spread over placebo and filgotinib groups. Consistent with its selective JAK1 inhibition, filgotinib treatment led to an improvement in hemoglobin (up to 0.5 g/dL, or a 4% increase from baseline). All lipid fractions including HDL and LDL increased, with the largest percentage increase in HDL. Lymphocytes were not impacted by treatment with filgotinib in this study. No clinically significant changes or discontinuations were observed for male reproductive hormones.
Galapagos announced topline results after 24 weeks of treatment in the DARWIN 2 trial in August 2015. DARWIN 2 was a 24-week, double-blind, placebo-controlled evaluation of filgotinib, as once-daily administration (QD dosing) at three dose levels. DARWIN 2 results were for 283 patients with moderate to severe RA who showed an inadequate response to MTX. Filgotinib or placebo was given as monotherapy. The patients were evaluated up to 24 weeks. Galapagos achieved the primary endpoint of ACR20 response with all three doses at 12 weeks and went on to report the following ACR50 responses at 12 and 24 weeks of once-daily monotherapy:
ACR50 Responses
DARWIN 2, ITT-NRI
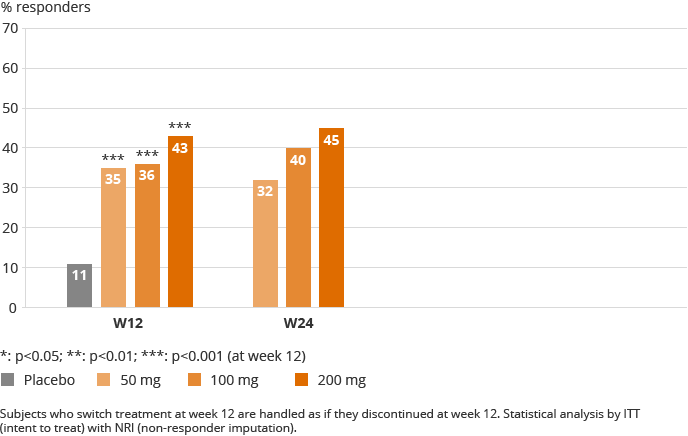

The results from DARWIN 2 showed a rapid onset of efficacy, as of week one for ACR and DAS28(CRP) responses. Maximum ACR20 and ACR50 responses were obtained at week eight and week twelve respectively. Additional gain was reported for ACR70 and DAS28 (CRP) during the second half of the study. In the highest dose groups, up to 50% of the patients reached low disease activity or remission.
Over all DARWIN 2 dose groups including placebo, 3.9% of patients stopped treatment during the study for safety reasons. A higher discontinuation rate for safety was observed for placebo (5.6%) during the first 12 weeks of the study compared to filgotinib treated patients (2.5%) up to week 24. Similar incidence of serious and non-serious treatment-emergent adverse events was reported, evenly spread over the dose groups including placebo. A higher rate of infections was observed in filgotinib (19% over 24 weeks) compared to placebo (10% up to week 12), with serious infections remaining limited (1.4% of filgotinib patients). No malignancies, tuberculosis, major adverse cardiac events, opportunistic infections, or deaths were reported. Consistent with its selective JAK1 inhibition, filgotinib treatment led to an improvement in hemoglobin (up to 0.4 g/dL, or 3.6% increase from baseline). Neutrophil levels remained stable after initial decline to mid-normal range at week four. There was no impact on lymphocytes or liver function tests. The similar increases in LDL and HDL were maintained. No clinically significant changes or discontinuations were observed for male reproductive hormones.