The potential of CFTR modulators for the treatment of CF
There is no cure for CF, and to date, all but one of the therapies approved to treat CF patients have been designed to treat the symptoms rather than address the underlying cause of the disease. The market for CF therapies, across the six main healthcare markets, exceeded $1 billion in 2012 and is to exceed $5 billion in 2018 according to a July 2014 GlobalData OpportunityAnalyzer report, primarily driven by introduction of disease modifying treatments. To treat the symptoms of disease, such as CF-associated malnutrition, diabetes, lung disease and systemic inflammation, an aggressive combination of specific therapies is required. To address the cause of the disease, the primary focus has been on a class of drugs known as CFTR modulators.
Two types of disease-modifying CFTR modulators are the primary area of focus for therapies under development. Potentiator molecules are designed to restore the flow of ions through an activated CFTR by influencing the channel’s open probability. Potentiator molecules can only function if CFTR is already present in the cell membrane (Class III/IV) mutations. Corrector molecules are designed to overcome defective protein processing by restoring proper folding of CFTR and allowing for increased surface expression (Class II mutations).
Kalydeco, marketed by Vertex, is currently the only approved therapy to address the cause of Class III mutation CF. Kalydeco is an orally-administered prescription CFTR potentiator for the treatment of patients two years of age and older with CF who have several specific mutations in the CFTR gene, including the Class III (G551D) mutation. Kalydeco is designed to keep the CFTR protein channels on the cell surface open longer in order to increase the flow of salt and water into and out of the cell. However, this treatment is limited to the subset of patients who suffer from the Class III and other gating mutations of the CFTR gene. Class III mutations occur in only a small percentage of patients with CF (4%).
In contrast, the Class II F508del mutation affects approximately 90% of all CF patients. In these patients, CFTR is not expressed at the cell surface and cannot be potentiated by drugs like Kalydeco (that can only function if CFTR is already present in the cell membrane). Small molecule corrector approaches aim to transport the non-functional Class II CFTR protein to the cell membrane. Lumacaftor (VX-809), which was developed by Vertex, is a small molecule corrector approved for patients with two copies (homozygous) of the Class II (F508del) mutation in their CFTR gene for use in combination with Kalydeco. Vertex refers to this combination of lumacaftor and Kalydeco as Orkambi, which is currently the only approved therapy to address the cause of Class II mutation CF. Orkambi showed statistically significant reductions in pulmonary exacerbations in the pooled analysis of the TRAFFIC and TRANSPORT Phase 3 studies. Other signs of clinical improvement were either limited or not statistically different from placebo.
The Class I mutations affect approximately 10% of all CF patients. This mutation shortens the length of the CFTR protein and leads to complete loss of CFTR function. To date, there are no approved molecules on the market to treat this mutation.
Despite the approval of Kalydeco and Orkambi, there is need for better therapies with improved pulmonary function. Though many pediatric patients have normal lung function at the time of diagnosis, physicians generally believe that earlier treatments can have downstream benefits for the patient by slowing the deterioration in lung function.
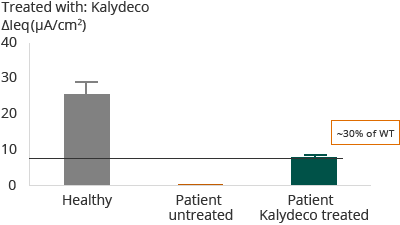
Galapagos believes that restoration of CFTR function in cellular assays may be predictive of clinical outcomes. Specifically, review of Vertex patient and cellular data has shown strong correlation as reflected in Diagram A. In the case of patients with F508del mutation, the administration of Kalydeco and lumacaftor combination resulted in approximately 20% restoration of normal, or wild-type, CFTR. The clinical outcome reflected in Vertex’s Phase 3 trial and primary endpoint was that 46% of patients showed an FEV1 improvement of greater than or equal to 5%. Forced expiratory volume (FEV1) levels are a measurement of the volume of air that can be forcibly blown out in one second after full inspiration. Further, as reflected in Diagram B, for patients with G551D mutation, the administration of Kalydeco resulted in approximately 30% restoration of wild-type CFTR. The clinical outcome reflected in Vertex’ Phase 3 trial and primary endpoint was that 75% of patients showed an FEV1 improvement of greater than or equal to 5%.
Diagram A
F508del – Homozygous for F508del
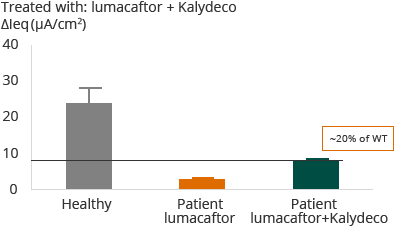

Diagram B
G551D – Heterozygous G551D with F508del

Galapagos believes these studies demonstrate that cellular models can be used to identify novel molecules to treat Class II and Class III mutations and select those combinations that can restore wild-type CFTR to greater than 50%, a threshold that we believe needs to be achieved to lead to disease remission in patients.